
Effet de l’ADR-4 sur le fonctionnement du rein
ADR-4 – Effect on Kidney Functioning
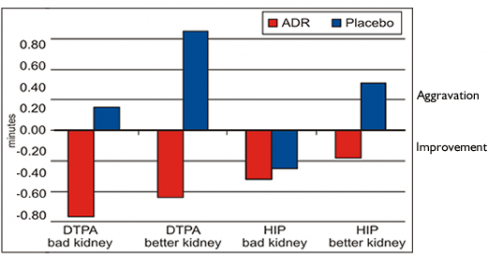
Mean kidney transport time in groups of persons using an active ADR products unit and inactive dummy (placebo). The negative sign stands for a reduction in the mean kidney transport time and signifies an improvement of kidney function.
The Renocystographic Assessment of the Effects of the ADR-4 Energy Stimulator on Kidney Functioning in Persons with Dysfunctional Kidneys
Authors: Prof. Szczesny Gorski, Phd. Stanislaw Wosinski, Prof. Wojciech Suwala, Prof. Bogumir Grala
Summary
The aim of the research was to investigate possible changes in the functioning of impaired kidneys under the application of the magnetic water energy stimulator ADR-4. Quantitative (32 parameters) filtration-extraction renographic evaluation of kidney functioning using DTPA Tc 99m and I125 hippurate was performed, according to our own standard methodology, on persons referred by hospital departments and clinics, recruited according to current submission order. The evaluation was done on a double blind principle in two groups with moderate and considerable kidney function impairment, as assessed by initial renography: 17 women and 4 men aged 18-84 years, using an active ADR-4 for one month; and 8 women and 4 men aged 26-60 years, using an inactive dummy of the same size, colour and weight, for the same period, in compliance with the producer’s instructions. The renography examination was then repeated. The subsequent statistical analysis (Student’s t-test) compared the results obtained in the two groups during the initial and final tests, separately for kidneys which the initial test found to be functioning better or worse. In the case of renographic parameters for which positive differences were noted in the ADR-4 group and negative differences in the placebo group, the Wilks lambda test was then additionally applied.
The results of the statistical evaluation confirmed the beneficial effects of using the ADR-4 energy stimulator on several kidney functions: diuresis, filtration, extraction and excretion; the mean DTPA transport time was also reduced. This positive evaluation is enhanced by the observation that in the group using the placebo the results were unchanged or poorer on the second term of measurement, after one month. In conclusion, evidence was gained of the positive effects of using the ADR-4, over a one-month period, on kidneys with moderately and significantly impaired functioning.
Introduction
The use of filtration-extraction renocystography in the assessment of kidney functioning has been an indisputable application of this method for many years. Our own computerised, quantitative filtration-extraction renography, elaborated over many years of practical use, allows one to carry out an initial, yet relatively precise and comprehensive, quantitative and qualitative, evaluation of the functioning of kidneys and of the lower urinary tracts. Among other things, the measurement system provides indices of glomerular and tubular clearance, filtration fraction for both kidneys separately or together, mean time of renal filtration and extraction transit, excretion indices at 10, 15 and 30 minutes, respective norms, the residual volume of urine in the bladder in percentages and in cubic centimetres and a mean diuresis, calculated in strictly standardised water load, evaluated with account taken of current blood pressure altogether 32 quantitative parameters (Górski 1994). The sensitivity of the renographic procedure which we apply is approx. 98% (Goris 1985).
It is useful as an initial method, particularly in the examination of patients with arterial hypertension, with the use of the captopril test for the detection of renal arterial stenosis, in cases of glomerulitis and/or pyelitis, in renal and cystic tract calculi, in assessing the degree of evacuation from the bladder, and in cases of pains of obscure etiology in the lumbar region.
The aim of the present research was to test for possible changes in the functioning of kidneys, evaluated using this method, during treatment with the magnetic energy stimulator invented by one of the authors (S. Wosi?ski).
The ADR-4 is an energy stimulator registered with the Polish Patents Office under the number P320179[5]. This stimulator takes the form of a polygonal disc. At the base of the disc is a ceramic element, on top of which are placed magnetic elements of various intensity and specific dimensions, which provide the requisite spatial configuration of a stable, heterogeneous magnetic field. The task of the ADR-4 is to improve the sanitary properties of both pure water and water contained in various aliments. We know that water can, for a certain time, possess altered properties, e.g. surface tension, relative permittivity, electric conductivity, and NMR, NQR, UV and IR spectra, under the influence of certain activity, such as electromagnetic fields. These altered properties in water have a certain effect on living organisms, from bacteria to man. Research is currently in progress into the effects of the ADR-4 on the speed in which free radicals are scavenged from aqueous solutions[6].
Materials and Research Methods
The ADR-4 stimulators were obtained from the producer[7].
The renographic tests were carried out using the computerised renocystograph RENOMIC II[8], constructed by a team led by one of the authors (S.G.). The research was made on two randomly-chosen groups of patients, referred by hospital departments and clinics, in which initial tests showed moderately or seriously impaired functioning of one or both kidneys, as assessed according to our own renographic classification. After eliminating subjects who did not present themselves for the second series of tests and those whose results were invalid for technical reasons, there remained 33 individuals. Of these, 21 (17 women and 4 men, aged from 18 to 84, av. 43, S.D. 15.4 years) subsequently used an active ADR-4 over a period of one month, in accordance with the producer’s instructions, and the remaining 12 subjects (8 women and 4 men, aged from 26 to 60, av. 48, S.D. 10 years) used an inactive dummy weighing and looking the same as the active ADR-4. Neither the patients nor the personnel carrying out the research, including the person describing the tests, knew which kind of disc had been used until the second series of tests had been completed and described. The technical factors which excluded certain results were the following: the failure to provide urine for the second test, a mean blood pressure below 95 mm, a difference of 5? C or more in the ambient temperature between the two test terms, the discontinuing or commencement during the testing period of new nephroleptic medicines or of strong general medicines, e.g. antibiotics, and the appearance of acute additional pathologies, e.g. renal colic with blockage of the kidney.
Methodology of the Statistical Analysis
Applied for all the noted indices of the work of the kidneys was a statistical evaluation based on the Student’s t-test for the paired variables method. This involves, for each index, subtracting from the value noted for test II the result of test I (carried out before the disc was applied). Next, the value of the mean difference and the evaluation of its standard error were indicated for each index in both groups. The quotient of the mean difference obtained through the evaluation of its standard error has the Student’s t-distribution with the number of independent variables equal to no 1, where n is the number of individuals observed in a group. The results are presented in table 1.
A separate explanation is required for the method of inference applied. For the majority of indices (with the exception of T max and of systolic and diastolic blood pressure, the values of which, both high and low, are negative), one can take as favourable a rise in their value. If, therefore, the ADR-4 stimulators fail to act in a positive manner on the functioning of the kidneys, the mean difference between measurements II and I should be negative (deterioration) or close to zero (no change).
The (unilateral) null hypothesis should thus read as follows:
Ho: the mean difference of a given index is less than or equal to zero.
The alternative hypothesis, meanwhile,
H1: the mean difference of a given index is greater than zero.
If, therefore, the value of the unilateral Student’s test will exceed the critical value by an appropriate amount, we will reject the null hypothesis of the lack of any effect on the part of the ADR-4 on the given index of the work of the kidneys.
For indices whose improvement occurs with a fall in their value, the null hypothesis will be rejected if the result of the unilateral test is negative and, simultaneously, greater, in terms of absolute value, than the critical value.
It should be emphasised that the most commonly published tables of critical values of a Student’s test serve to verify bilateral hypotheses; hence, in reading from them critical values for the verification of unilateral hypotheses, one must allow for a significance level twice as great as that which we apply. The critical values necessary for the evaluation of the test are given below the tables of results.
When making inference, a maximum significance level of 0.10 has been adopted. If the value of the Student test exceeds the critical value read with this significance level, then we reject the null hypothesis of a lack of any effect on the part of the ADR-4 on the particular renal index, in which case the rejection risk of the null hypothesis does not exceed 10% (i.e. 0.1). For a considerable number of indices, the rejection of the null hypothesis of the lack of effect of the ADR-4 was possible at an even lower significance level; this has been expressed in the table.
In order to effect a simultaneous evaluation of the positive rise in the value of some of the indices in the ADR group against a fall in their value in the placebo group, the Wilkslambda test was additionally applied. The results have been included in table 2, following the transformation of the statistics of the Wilks lambda test into F. Fisher statistics.
Results and Discussion
For indices such as volume of urine excreted, total excretion and diuresis, substantially favourable changes were noted in the ADR group and substantially unfavourable changes in the placebo group. Moreover, in the case of the placebo there occurred a substantial reduction in residual volume, and a substantial change in the participation of both worse and better kidneys in filtration (the participation of the worse kidney rose substantially – to 50 %).
There was also a substantial improvement in the due excretion of DTPA in the ADR group for the better kidney, constituting a measure of the due capture (N) of the tracer; in the placebo group, meanwhile, there was a substantial decrease in the excretion of DTPA for the better kidney (both due (N) and actual (R) excretion). There was also an improvement in some of the indices of the excretion of hippurate in the ADR group.
All the indices of the outflow of both DTPA and hippurate, for the worse and the better kidneys in the ADR group, showed a substantial improvement after 10 and 15 minutes.
Meanwhile, the time T max, representing the measure of the mean transit time of the tracer through the kidney, lessened substantially in the case of DTPA in the ADR group (which is favourable), and grew in the placebo group (which is unfavourable). One may thus advance the general conclusion that the results in the two groups logically complement one another (in the placebo group the substance of the null and alternative hypotheses should be exchanged with one another, since where the ADR fails to act and an illness is present the indices may worsen or at best remain unchanged).
In order to avoid any suspicions that, although the subjects were assigned to the two groups in a random manner, significant differences could have appeared between the groups, a Student’s test was carried out to compare the mean values of the indices for both groups. Substantial differences (in the case of bilateral hypotheses) were noted for the following indices (table 2):
residual volume in term 1 (ADR > placebo),
contribution of the worse kidney to extraction in term I (ADR < placebo),
contribution of the better kidney to extraction in term I (ADR > placebo),
contribution of the worse kidney to filtration in term II (ADR < placebo),
contribution of the better kidney to filtration in term II (ADR > placebo),
contribution of the worse kidney to extraction in term II (ADR < placebo),
contribution of the better kidney to extraction in term II (ADR > placebo),
excretion of DTPA by the better kidney in term II (ADR > placebo), both due (N) and actual (R),
excretion of HIP by the better kidney in term II (ADR > placebo), both N and R.
However, the substantial differences revealed signify that the state of the subjects from the ADR group was (in terms of these indices) significantly worse than in the placebo group. In spite of this, an improvement occurred in a range of indices in the ADR group, and in the placebo group – a deterioration.
Also tested was the asymmetry in the functioning of the kidneys (tab. 3). For the indices measured for both kidneys, the differences between the better and the worse kidney were indicated and subjected to statistical analysis using a Student’s test for the paired variables method. Striking here is the lack of a substantial difference for the excretion index of DTPA and for the index T max for DTPA and (in part) hippurate. For the remaining indices, significant differences were noted (higher values for the better kidney, except in the case of the index of filtration, where the reverse was shown).
The observed changes in blood pressure can be deemed incidental: after age is accounted for, the differences fall within the norms. The R/R age norms are taken from the Ciba-Geigy tables (Diem 1972).
The results of the evaluation of the positive rise in the value of some of the indices in the ADR group against a fall in their value in the placebo group, effected using the Wilks lambda test (Grala, 1975), have been included in table 2, following the transformation of the statistics of the Wilks lambda test into F. Fisher statistics. On the graph, they correspond to the positive columns for the ADR group and the negative columns for the placebo group.
Substantial differences were noted for the following indices:
total volume,
diuresis,
residual volume,
DTPA excretion for the better kidney (N and R),
DTPA outflow for the worse kidney (R only),
T max for DTPA for the better kidney.
Conclusions
The results obtained confirm the positive effects of the application of the ADR-4 on the functioning of kidneys impaired to a moderate or considerable degree.
The above conclusion is enhanced by the fact that in the group of individuals using the inactive dummy the indices either remained unchanged or underwent a significant deterioration, as well as by the fact that the initial results in the ADR group indicated a significantly worse functioning of the kidneys than in the placebo group.
One should point out that increasing the number of subjects observed in the two groups could provide more clear-cut results. A longer period of application of the ADR-4 could probably also bring more pronounced results. In order to verify this assumption, research is currently under way into the same persons – after a year of using the ADR-4.
Literature
Diem K, Lentner C.: Tables scientifiques, VII edition, Ciba-Geigy, Basel, 1972, p. 564
Goris M.L.: Sensitivity and specifity of common scintigraphic procedures. Year Book Medical Publishers, Chicago, 1985, 48
Gorski Sz.: Computerized renocystography for quantitative filtration – extraction. Nucl. Med. Comm. 1994, 15:182-187
Grala B. Wietlicka – Grala J., Wojtaszek J.: Analiza krzywych reakcji ilosciowych w badaniach hemodynamicznych. Listy Biometryczne. 1975, 46, I – 22
Radiophysical Laboratory of the Institute of Radiology of the Faculty of Medicine in Poznan
ADR SYSTEM Gdansk
Kidney Disease Clinic of the Group of Specialist Clinics in Poznan
Centre for Information on Scientific, Technical and Economic Matters and Patents of the Institute of Natural Fibres in Poznan
The ADR-4 stimulator was awarded the Gold Medal with special distinction at the 47th World Exhibition of Innovation, Inventions and New Technologies BRUSSELS EUREKA 1998, the Grand Prix at the International Exhibition of Inventors INPEX 2001 in Pittsburgh PE, USA, and the Gold Medal at the WORLD GENIUS CONVENTION 2001 in Tokyo
Scavenging of free radicals from DTPH by antioxidants such as eg, Roibos and Green tea water drinking infusions. EPR Laboratory of the Institute of Physics of Adam Mickiewicz University in Poznan
RENOMIC II was awarded the Gold Medal at the BRUSSELS EUREKA 2000 exhibition
